What is childhood thyroid cancer?
Thyroid cancer in children is a rare cancer that forms in the thyroid, a butterfly-shaped gland at the base of the throat near the windpipe (also called the trachea). The thyroid gland has a right lobe and a left lobe that is connected by a thin piece of tissue called the isthmus. Although thyroid cancer can affect children of all ages, it's more common in adolescents and girls. It also occurs more often in White people than in Black people.
Children can also have thyroid nodules. A thyroid nodule is an abnormal growth of thyroid cells in the thyroid. The nodules may be solid or fluid-filled. Thyroid nodules usually don't cause symptoms or need treatment unless they become large enough that it is hard to swallow or breathe. Only one in five thyroid nodules become cancer.
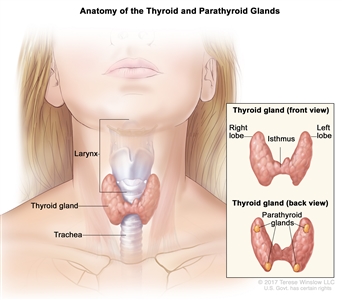
Anatomy of the thyroid and parathyroid glands. The thyroid gland lies at the base of the throat near the trachea. It is shaped like a butterfly, with the right lobe and left lobe connected by a thin piece of tissue called the isthmus. The parathyroid glands are four pea-sized organs found in the neck near the thyroid. The thyroid and parathyroid glands make hormones.
The thyroid uses iodine, a mineral found in some foods and in iodized salt, to help make several hormones. Thyroid hormones:
- control heart rate, body temperature, and how quickly food is changed into energy (metabolism)
- control the amount of calcium in the blood
Types of childhood thyroid cancer
There are four types of thyroid cancers:
-
Papillary thyroid carcinoma is the most common type of thyroid cancer in children, occurring most often in teens. It usually affects both sides of the thyroid and often spreads to lymph nodes in the neck and sometimes the lungs.
-
Follicular thyroid carcinoma usually forms in one area of the thyroid. It often spreads to the bone and lung but rarely spreads to the lymph nodes in the neck.
-
Medullary thyroid cancer forms from parafollicular C cells in the thyroid. It is usually linked to a certain inherited change in the RET gene and multiple endocrine neoplasia type 2 (MEN 2) syndrome. It occurs most often in children aged 4 years and younger and may have spread to other parts of the body at the time of diagnosis. Children who have MEN2 syndrome may also be at risk of developing pheochromocytoma or hyperparathyroidism.
- Anaplastic thyroid cancer rarely occurs in children. To learn more, see Anaplastic Thyroid Cancer (ATC).
Papillary and follicular thyroid cancer are sometimes called differentiated thyroid cancer. Medullary and anaplastic thyroid cancer are sometimes called poorly differentiated or undifferentiated thyroid cancer.
Adenomas are a type of thyroid nodule that can grow very large and sometimes make hormones. Adenomas are not cancer but may rarely become cancer and spread to the lungs or lymph nodes in the neck.
Causes and risk factors for childhood thyroid cancer
Thyroid cancer in children is caused by certain changes to the way thyroid cells function, especially how they grow and divide into new cells. Often, the exact cause of these cell changes is unknown. To learn more about how cancer develops, see What is Cancer?
A risk factor is anything that increases the chance of getting a disease. Not every child with one or more of these risk factors will develop thyroid cancer. And it will develop in some children who don't have a known risk factor.
Risk factors for childhood thyroid cancer include:
- being exposed to radiation, such as from diagnostic tests, radiation treatment, or radiation in the environment
- having autoimmune thyroiditis
- having certain genetic syndromes, such as:
- multiple endocrine neoplasia type 2A (MEN2A) syndrome
- multiple endocrine neoplasia type 2B (MEN2B) syndrome
- having a family history of thyroid cancer, including:
- APC-associated polyposis
- DICER1 syndrome
- Carney complex
- PTEN hamartoma tumor syndrome
- Werner syndrome
Talk with your child's doctor if you think your child may be at risk for thyroid cancer.
Genetic counseling for children with thyroid cancer
It is not always clear from the family medical history whether a condition is inherited. Genetic counseling can assess the likelihood that your child's cancer is inherited and whether genetic testing is needed. Genetic testing may help explain why a child develops a rare cancer or a cancer that is usually seen in adults. Genetic counselors and other specially trained health professionals can discuss your child's diagnosis and family medical history to help you understand:
- the options for testing for changes in the RET, DICER1, or APC gene
- the risk of other cancers for your child
- the risk of thyroid cancer or other cancers for your child's siblings
- the risks and benefits of learning genetic information
Genetic counselors can also help you cope with your child's genetic testing results, including how to discuss the results with family members. They can also advise you about whether other members of your family should receive genetic testing.
If your child has been found to have a change in the RET gene, other family members may also be tested to find out if they have an increased risk of medullary thyroid cancer. Family members, including young children, who have the changed gene may have a thyroidectomy (surgery to remove the thyroid). This can decrease the chance of developing medullary thyroid cancer.
Learn more about Genetic Testing for Inherited Cancer Risk.
Symptoms of childhood thyroid cancer
Often thyroid cancer is found when a physical exam or an imaging test is done for another health problem. Sometimes the cancer can cause symptoms. It's important to check with your child's doctor if your child has:
- a lump in the neck
- trouble breathing
- trouble swallowing
- hoarseness or a change in the voice
Children with changes to the RET gene may have symptoms that can lead to an early diagnosis of multiple endocrine neoplasia type 2A or 2B syndrome. It's important to check with your child's doctor if your child has:
- bumps on the lips, tongue, or eyelids that do not hurt
- trouble making tears
- constipation
- Marfan syndrome (being tall and thin, with long arms, legs, fingers, and toes)
These symptoms may be caused by problems other than thyroid cancer. The only way to know is to see your child's doctor.
Tests to diagnose childhood thyroid cancer
If your child has symptoms that suggest thyroid cancer, the doctor will need to find out if these are due to cancer or to another problem. They will ask when the symptoms started and how often your child has been having them. They will also ask about your child's personal and family medical history and do a physical exam. Depending on these results, they may recommend other tests. If your child is diagnosed with thyroid cancer, the results of these tests will help you and your child's doctor plan treatment.
The tests used to diagnose thyroid cancer may include:
Thyroid function test
A thyroid function test checks the blood for abnormal levels of thyroid-stimulating hormone (TSH). TSH is made by the pituitary gland in the brain. It stimulates the release of thyroid hormone and controls how fast follicular thyroid cells grow. The blood may also be checked for high levels of calcitonin (a hormone made by the thyroid that decreases the amount of calcium in the blood).
Thyroglobulin test
A thyroglobulin test checks the blood for the amount of thyroglobulin, a protein made by the thyroid gland. Thyroglobulin levels are low or absent with normal thyroid function but may be higher with thyroid cancer or other conditions.
RET,DICER1, orAPCgenetic testing
A RET, DICER1, or APC genetic test checks a sample of blood, saliva, or tissue for certain changes in the RET, DICER1, or APC genes.
Ultrasound
An ultrasound exam uses high-energy sound waves (ultrasound) that bounce off internal tissues or organs in the neck and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure can show the size of the mass and whether it is solid or a fluid-filled cyst. Ultrasound may be used to guide a fine-needle aspiration biopsy. A complete ultrasound exam of the neck is done before surgery.
Thyroid scan
A thyroid scan uses a small amount of a radioactive substance that is swallowed or injected. The radioactive material collects in thyroid gland cells. A special camera linked to a computer detects the radiation given off and makes pictures that show how the thyroid looks and functions and whether the cancer has spread beyond the thyroid gland. If the amount of TSH in the child's blood is low, a scan to make images of the thyroid may be done before surgery.
CT scan (CAT scan)
A CT scan uses a computer linked to an x-ray machine to make a series of detailed pictures of areas inside the body, such as the neck, chest, abdomen, and brain. The pictures are taken from different angles and are used to create 3-D views of tissues and organs. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography. To learn more, see Computed Tomography (CT) Scans and Cancer.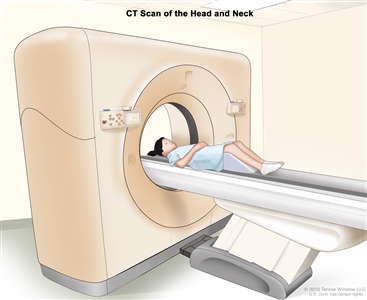
Computed tomography (CT) scan of the head and neck. The child lies on a table that slides through the CT scanner, which takes a series of detailed x-ray pictures of the inside of the head and neck.
Magnetic resonance imaging (MRI) with gadolinium
MRI uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the neck and chest. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Chest x-ray
An x-ray is a type of radiation that can go through the body and make pictures. A chest x-ray makes pictures of the organs and bones inside the chest.
Biopsy
Biopsy is a procedure in which a sample of tissue is removed from the tumor so that a pathologist can view it under a microscope to check for signs of cancer.
-
Fine-needle aspiration biopsy is the removal of thyroid tissue using a thin needle. The needle is inserted through the skin into the thyroid. Several tissue samples are removed from different parts of the thyroid. A pathologist views the tissue samples under a microscope to look for cancer cells. If it is not clear whether cancer is present, a surgical biopsy may be done.
-
Surgical biopsy is the removal of the thyroid nodule or one lobe of the thyroid during surgery so the cells and tissues can be viewed under a microscope by a pathologist to check for signs of cancer.
Whole-body thyroid scan
A whole-body thyroid scan uses a small amount of radioactive substance that is swallowed or injected. The radioactive material collects in any thyroid tissue or cancer cells remaining after surgery. Radioactive iodine is used because only thyroid cells take up iodine. A special camera detects the radiation given off by the thyroid tissue or cancer cells. This procedure is also called radioactive iodine scan or RAI scan.
Getting a second opinion
You may want to get a second opinion to confirm your child's cancer diagnosis and treatment plan. If you seek a second opinion, you will need to get medical test results and reports from the first doctor to share with the second doctor. The second doctor will review the genetic test report, pathology report, slides, and scans. This doctor may agree with the first doctor, suggest changes to the treatment plan, or provide more information about your child's cancer.
To learn more about choosing a doctor and getting a second opinion, see Finding Cancer Care. You can contact NCI's Cancer Information Service via chat, email, or phone (both in English and Spanish) for help finding a doctor or hospital that can provide a second opinion. For questions you might want to ask at your child's appointments, see Questions to Ask Your Doctor about Cancer.
Who treats children with thyroid cancer?
A pediatric oncologist, a doctor who specializes in treating children with cancer, oversees treatment of thyroid cancer. The pediatric oncologist works with other health care providers who are experts in treating children with cancer and who specialize in certain areas of medicine. Other specialists include:
- pediatrician
- pediatric surgeon
- radiation oncologist
- pathologist
- pediatric nurse specialist
- social worker
- rehabilitation specialist
- psychologist
- child-life specialist
Types of treatment for childhood thyroid cancer
There are different types of treatment for children and adolescents with thyroid cancer. You and your child's cancer care team will work together to decide treatment. Many factors will be considered, such as your child's overall health and whether the tumor is newly diagnosed or has come back.
Your child's treatment plan will include information about the cancer, the goals of treatment, treatment options, and the possible side effects. It will be helpful to talk with your child's cancer care team before treatment begins about what to expect. For help every step of the way, see our booklet, Children with Cancer: A Guide for Parents.
Treatment for thyroid cancer might include:
Surgery
Surgery is the most common treatment for thyroid cancer. One of the following procedures may be used:
- Total thyroidectomy is the removal of the whole thyroid. Lymph nodes near the cancer may also be removed and checked under a microscope for signs of cancer.
- Near-total thyroidectomy is the removal of all but a very small part of the thyroid. Lymph nodes near the cancer may also be removed and checked under a microscope for signs of cancer.
In children, a total thyroidectomy is usually done.
Learn more about Surgery to Treat Cancer.
Radioactive iodine therapy
Follicular and papillary thyroid cancers are sometimes treated with radioactive iodine (RAI) therapy. RAI therapy may be given to children after surgery to kill any thyroid cancer cells that were not removed or to children whose tumor cannot be removed by surgery. RAI is taken by mouth and collects in any remaining thyroid tissue, including thyroid cancer cells that have spread to other places in the body. Because only thyroid tissue takes up iodine, the RAI destroys thyroid tissue and thyroid cancer cells without harming other tissue. Before a full treatment dose of RAI is given, a small test dose is given to see if the tumor takes up the iodine.
Targeted therapy
Targeted therapy uses drugs or other substances to block the action of specific enzymes, proteins, and other molecules involved in the growth and spread of cancer cells. Targeted therapies used to treat thyroid cancer include:
- entrectinib
- larotrectinib
- selpercatinib
- vandetanib
Targeted therapy is being studied for the treatment of childhood thyroid cancer that has recurred (come back).
Learn more about Targeted Therapy to Treat Cancer.
Clinical trials
Joining a clinical trial may be an option. There are different types of clinical trials for childhood cancer. For example, a treatment trial tests new treatments or new ways of using existing treatments. Supportive care and palliative care trials look at ways to improve quality of life, especially for those who have side effects from cancer and its treatment.
You can use the clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. The search allows you to filter trials based on the type of cancer, your child's age, and where the trials are being done.
To learn more, see Clinical Trials Information for Patients and Caregivers.
Treatment of newly diagnosed childhood papillary and follicular thyroid cancer
Treatment of papillary and follicular thyroid carcinoma in children may include:
- Surgery to remove all or most of the thyroid gland and sometimes lymph nodes near the thyroid gland. Radioactive iodine therapy may also be given if any thyroid cancer cells remain after surgery. Hormone replacement therapy (HRT) is given to make up for the lost thyroid hormone.
- Radioactive iodine therapy alone may be given to children whose tumor cannot be removed by surgery. HRT is given to make up for the lost thyroid hormone.
Treatment of newly diagnosed childhood medullary thyroid cancer
Treatment of medullary thyroid cancer in children may include:
- surgery to remove the cancer
- targeted therapy (selpercatinib or vandetanib) for cancer that has continued to grow during treatment or has spread to other parts of the body
Treatment of progressive or recurrent childhood thyroid cancer
Treatment of progressive or recurrent papillary and follicular thyroid carcinoma in children may include:
- radioactive iodine therapy
- targeted therapy (entrectinib, larotrectinib, or selpercatinib)
- a clinical trial of targeted therapy (selpercatinib)
Treatment of progressive or recurrent medullary thyroid cancer in children may include:
- a clinical trial of targeted therapy (selpercatinib)
Prognosis and prognostic factors for childhood thyroid cancer
If your child has been diagnosed with thyroid cancer, you likely have questions about how serious the cancer is and your child's chances of survival. The likely outcome or course of a disease is called prognosis.
The prognosis depends on:
- your child's age at the time of diagnosis
- the type of thyroid cancer
- the size of the cancer
- whether the tumor has spread to the lymph nodes or other parts of the body at the time of diagnosis
- whether the cancer was completely removed by surgery
The prognosis for most children with papillary thyroid cancer and follicular thyroid cancer is very good.
No two people are alike, and responses to treatment vary greatly. Your child's cancer care team is in the best position to talk with you about your child's prognosis.
Side effects and late effects of treatment
Cancer treatments can cause side effects. Which side effects your child might have depends on the type of treatment they receive, the dose, and how their body reacts. Talk with your child's treatment team about which side effects to look for and ways to manage them.
To learn more about side effects that begin during treatment for cancer, visit Side Effects.
Problems from cancer treatment that begin 6 months or later after treatment and continue for months or years are called late effects. Late effects of cancer treatment for childhood thyroid cancer may include:
- changes in the salivary glands
- increased risk of infection
- trouble breathing
- changes in mood, feelings, thinking, learning, or memory
- second cancers (new types of cancer)
Some late effects may be treated or controlled. It is important to talk with your child's doctors about the effects cancer treatment can have on your child. To learn more, see Late Effects of Treatment for Childhood Cancer.
Follow-up care
It is common for thyroid cancer to recur (come back), especially in children younger than 10 years and those with cancer in the lymph nodes. Ultrasound, whole-body scan, and thyroglobulin tests may be done from time to time to check if the cancer has recurred. Lifelong follow-up of thyroid hormone levels in the blood is needed to make sure the right amount of hormone replacement therapy (HRT) is being given. Talk with your child's doctor to find out how often these tests need to be done.
Related resources
For more childhood cancer information and other general cancer resources, see:
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute's (NCI's) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government's center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of childhood thyroid cancer. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary ("Updated") is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Pediatric Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become "standard." Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI's website. For more information, call the Cancer Information Service (CIS), NCI's contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as "NCI's PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary]."
The best way to cite this PDQ summary is:
PDQ® Pediatric Treatment Editorial Board. PDQ Childhood Thyroid Cancer. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/thyroid/patient/child-thyroid-treatment-pdq. Accessed <MM/DD/YYYY>.
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website's E-mail Us.
Last Revised: 2024-07-23
If you want to know more about cancer and how it is treated, or if you wish to know about clinical trials for your type of cancer, you can call the NCI's Cancer Information Service at 1-800-422-6237, toll free. A trained information specialist can talk with you and answer your questions.

