Our Health Library information does not replace the advice of a doctor. Please be advised that this information is made available to assist our patients to learn more about their health. Our providers may not see and/or treat all topics found herein.
Gastric Cancer Treatment: Treatment - Patient Information [NCI]
What Is Stomach Cancer?
Stomach (gastric) cancer is cancer that starts in the cells lining the stomach. The stomach is an organ on the left side of the upper abdomen that digests food. The stomach is part of the digestive tract, a series of hollow, muscular organs joined in a long, twisting tube from the mouth to the anus. The digestive tract processes nutrients in foods that are eaten and helps pass waste material out of the body:
- Food moves from the throat to the stomach through a tube called the esophagus.
- After food enters the stomach, it is broken down by stomach muscles that mix the food and liquid with digestive juices.
- After leaving the stomach, partly digested food passes into the small intestine and then into the large intestine.
- The end of the large intestine, called the rectum, stores the waste from the digested food until it is pushed out of the anus during a bowel movement.
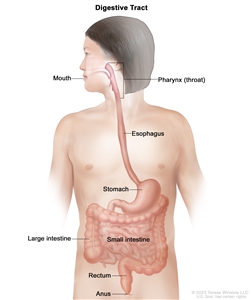
Anatomy of the digestive tract. The digestive tract is made up of organs that food and liquids travel through when they are swallowed, digested, absorbed, and leave the body as feces. These organs include the mouth, pharynx (throat), esophagus, stomach, small intestine, large intestine, rectum, and anus.
Types of stomach cancer
Adenocarcinoma of the stomach begins in the mucus-producing cells in the innermost lining of the stomach. Nearly all stomach cancers are adenocarcinomas.
Adenocarcinoma of the stomach is divided into two main classes, depending on where it forms in the stomach:
- Gastric cardia cancer begins in the top inch of the stomach, just below where it meets the esophagus.
- Non-cardia gastric cancer is cancer that begins in all other sections of the stomach.
Adenocarcinoma of the stomach also may be described as intestinal or diffuse, depending on how the cells look under a microscope:
- Intestinal adenocarcinomas are well differentiated, meaning the cancer cells look similar to normal cells under a microscope.
- Diffuse adenocarcinomas are undifferentiated or poorly differentiated, meaning the cancer cells look different from normal cells under a microscope. Diffuse adenocarcinomas tend to grow and spread more quickly than the intestinal type and be harder to treat.
Gastroesophageal junction adenocarcinoma (GEJ) is a cancer that forms in the area where the esophagus meets the gastric cardia. GEJ may be treated similarly to stomach cancer or esophageal cancer.
Gastrointestinal neuroendocrine tumors are cancers that begin in neuroendocrine cells (a type of cell that is like a nerve cell and a hormone-making cell) that line the gastrointestinal tract. Neuroendocrine cells make hormones that help control digestive juices and the muscles used in moving food through the stomach and intestines. Learn about gastrointestinal neuroendocrine tumors.
Gastrointestinal stromal tumors (GIST) begin in nerve cells that are found in the wall of the stomach and other digestive organs. GIST is a type of soft tissue sarcoma. Learn about gastrointestinal stromal tumors.
Primary gastric lymphoma is a type of non-Hodgkin lymphoma that forms in the stomach. Most primary gastric lymphomas are either mucosa-associated lymphoid tissue (MALT) gastric lymphoma or diffuse large B-cell lymphoma of the stomach.
Rarely, other types of cancer, such as squamous cell carcinoma, small cell carcinoma, and leiomyosarcoma, can also begin in the stomach.
Stomach Cancer Diagnosis
If you have symptoms that suggest stomach cancer, your doctor will need to find out if they're due to cancer or another condition. They may
- ask about your personal and family medical history to learn about your possible risk factors for stomach cancer
- do a physical exam, which will include feeling your abdomen for anything abnormal
- run blood tests to check for anemia (a low red blood cell count), which could be a sign of bleeding in the stomach
- check your stool for hidden (occult) blood, which could be a sign of bleeding in the stomach
Depending on these results, your doctor may recommend tests to find out if you have stomach cancer.
Tests to diagnose stomach cancer
The following tests and procedures are used to diagnose stomach cancer. The results will also help you and your doctor plan treatment.
Upper endoscopy with biopsy
Upper endoscopy is a procedure to look inside the esophagus, stomach, and duodenum (first part of the small intestine) to check for abnormal areas. An endoscope (a thin, lighted tube) is passed through the mouth and down the throat into the esophagus. It may also have a tool to remove a sample of cells or tissue (biopsy) so a pathologist can view it under a microscope to check for signs of cancer.
The sample of tissue may be checked for Helicobacter pylori (H. pylori) infection and used for biomarker testing.
Talk with your doctor to learn what to expect during and after your biopsy.
To learn about the type of information that can be found in a pathologist's report about the cells or tissue removed during a biopsy, see Pathology Reports.
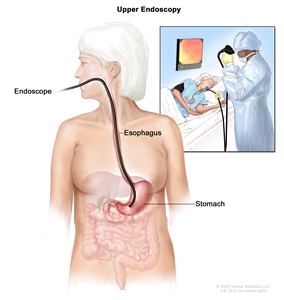
Upper endoscopy. A thin, lighted tube called an endoscope is inserted through the mouth and down the throat to check for abnormal areas in the esophagus, stomach, and first part of the small intestine.
Barium swallow
Barium swallow is a series of x-rays of the esophagus and stomach. The patient drinks a liquid that contains barium (a silver-white metallic compound). The liquid coats the esophagus and stomach, and x-rays are taken. This procedure is also called an upper GI series.
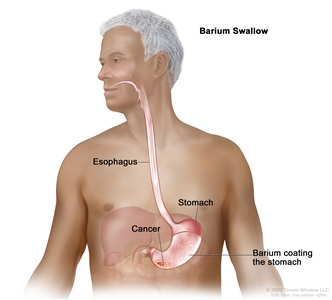
Barium swallow for stomach cancer. The patient drinks a liquid that contains barium (a silver-white metallic compound). The barium coats and outlines the inside of the esophagus and stomach. This allows abnormal areas, such as stomach cancer, to be seen on x-rays.
CT (CAT) scan
A CT scan uses a computer linked to an x-ray machine to make a series of detailed pictures of areas inside the body from different angles. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography. To learn more, see Computed Tomography (CT) Scans and Cancer.
Biomarker testing
Biomarker testing is a way to look for genes, proteins, and other substances (called biomarkers or tumor markers) that can provide information about cancer. Some biomarkers affect how certain cancer treatments work. Biomarker testing may help you and your doctor choose a cancer treatment for you.
To check for these biomarkers, samples of tissue containing stomach cancer cells are removed during a biopsy or surgery. The samples are tested in a laboratory to see whether the stomach cancer cells have these biomarkers.
For stomach cancer, biomarker testing includes the following:
- HER2: The cancer cells may have larger than normal amounts of a protein called HER2.
- PD-L1: The cells may have larger than normal amounts of an immune checkpoint protein called PD-L1.
- Microsatellite instability: The cells may have microsatellite instability. This may be caused by mistakes that don't get corrected when DNA is copied in a cell.
- Mismatch repair deficiency: The cells may have a defect in a mismatch repair gene.
- Tumor mutational burden: If the cells have a high tumor mutational burden, it means they have many gene mutations.
- NTRK : The cells may have changes in one of the NTRK genes.
Learn more about Biomarker Testing for Cancer Treatment.
Learn more about Stomach Cancer Treatment.
Tests to stage stomach cancer
If you're diagnosed with stomach cancer, you will be referred to a gastrointestinal oncologist. This is a doctor who specializes in diagnosing and treating cancers of the stomach and intestines. Your doctor will recommend tests to find out if the cancer has spread and if so, how far. Sometimes the cancer is only in the stomach. Or, it may have spread from the stomach to other parts of the body. The process of learning the extent of cancer in the body is called staging. It is important to know the stage of the stomach cancer to plan treatment.
The following imaging tests and procedures may be used to find out your stage:
- Endoscopic ultrasound is a procedure in which an endoscope is inserted into the body, usually through the mouth or rectum. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. A probe at the end of the endoscope is used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure is also called endosonography.
-
PET-CT scan combines the pictures from a positron emission tomography (PET) scan and a computed tomography (CT) scan. The PET and CT scans are done at the same time on the same machine. The pictures from both scans are combined to make a more detailed picture than either test would make by itself.
- For the PET scan, a small amount of radioactive glucose is injected into a vein. The scanner rotates around the body and makes a picture of where glucose is being used in the body. Cancer cells show up brighter in the picture because they are more active and take up more glucose than normal cells.
- For the CT scan, a series of detailed x-ray pictures of areas inside the body is taken from different angles. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly.
- Magnetic resonance imaging (MRI) with gadolinium is a procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Laparoscopy is a surgical procedure to look at the organs inside the abdomen to check for signs of disease. Small incisions (cuts) are made in the wall of the abdomen and a laparoscope (a thin, lighted tube) is inserted into one of the incisions. Other instruments may be inserted through the same or other incisions to perform procedures such as removing organs or taking tissue samples to be checked under a microscope for signs of cancer. A solution may be washed over the surface of the organs in the abdomen and then removed to collect cells. These cells are also looked at under a microscope to check for signs of cancer.
Getting a second opinion
You may want to get a second opinion to confirm your stomach cancer diagnosis and treatment plan. If you seek a second opinion, you will need to get important medical test results and reports from the first doctor to share with the second doctor. The second doctor will review the pathology report, slides, and scans before giving a recommendation. The doctor who gives the second opinion may agree with your first doctor, suggest changes or another approach, or provide more information about your cancer.
To learn more about choosing a doctor and getting a second opinion, see Finding Cancer Care. For questions you might want to ask at your appointments, see Questions to Ask Your Doctor about Cancer.
Stomach Cancer Stages
Cancer stage describes the extent of cancer in the body, such as the size of the tumor, whether it has spread, and how far it has spread from where it first formed. It is important to know the stage of the stomach cancer to plan the best treatment.
There are several staging systems for cancer that describe the extent of the cancer. Stomach cancer staging usually uses the TNM staging system. You may see your cancer described by this staging system in your pathology report. Based on the TNM results, a stage (I, II, III, or IV, also written as 1, 2, 3, or 4) is assigned to your cancer. When talking to you about your cancer, your doctor may describe it as one of these stages.
For information about how doctors stage stomach cancer, see the tests to stage stomach cancer section on Stomach Cancer Diagnosis. Learn more about Cancer Staging.
The information on this page is about staging for adenocarcinoma of the stomach, the most common type of stomach cancer.
Layers of the stomach wall
The stomach wall is made up of five layers of tissue and muscle. Knowing about these layers can help you understand the stage of your cancer.
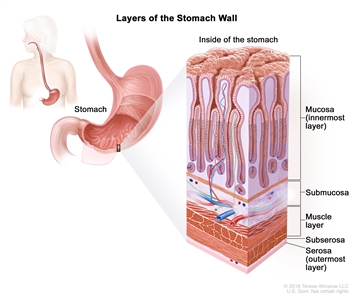
Layers of the stomach wall. The wall of the stomach is made up of the mucosa (innermost layer), submucosa, muscle layer, subserosa, and serosa (outermost layer). The stomach is an organ in the upper abdomen.
- The mucosa is the innermost layer of the stomach wall. It is made of both epithelial cells and glandular cells. The glandular cells make mucus to protect the stomach lining and digestive juices to help break down food. Most stomach cancers start in glandular cells of the mucosa. Cancers that start in glandular cells are adenocarcinomas.
- The submucosa is the layer of connective tissue between the mucosa and the muscle layer. It contains blood vessels, lymph vessels, and nerve cells.
- The muscle layer is the next layer. The muscle layer helps the stomach mix food with digestive juices and move it into the small intestine, where nutrients are absorbed.
- The subserosa is a thin layer of connective tissue between the muscle layer and the serosa.
- The serosa is the outermost layer of the stomach wall.
Stomach cancers become more advanced as they spread from the mucosa to the outer layers.
To learn more about the stomach, see What Is Stomach Cancer?
Stage 0 (carcinoma in situ) of the stomach
Stage 0 refers to carcinoma in situ. This means that abnormal cells are found in the mucosa. These abnormal cells may become cancer and spread into nearby normal tissue.
Learn about treatment of stage 0 (carcinoma in situ) of the stomach.
Stage I (also called stage 1) stomach cancer
Stage I is divided into stages IA and IB.
- In stage IA,
- cancer has formed in the mucosa and may have spread to the submucosa.
- In stage IB,
- cancer has formed in the mucosa and may have spread to the submucosa and has spread to 1 or 2 nearby lymph nodes; or
- cancer has formed in the mucosa and has spread to the muscle layer.
Learn about treatment of stage I stomach cancer.
Stage II (also called stage 2) stomach cancer
Stage II is divided into stages IIA and IIB.
- In stage IIA,
- cancer may have spread to the submucosa and has spread to 3 to 6 nearby lymph nodes; or
- cancer has spread to the muscle layer and to 1 or 2 nearby lymph nodes; or
- cancer has spread to the subserosa.
- In stage IIB,
- cancer may have spread to the submucosa and has spread to 7 to 15 nearby lymph nodes; or
- cancer has spread to the muscle layer and to 3 to 6 nearby lymph nodes; or
- cancer has spread to the subserosa and to 1 or 2 nearby lymph nodes; or
- cancer has spread to the serosa.
Learn about treatment of stage II stomach cancer.
Stage III (also called stage 3) stomach cancer
Stage III is divided into stages IIIA, IIIB, and IIIC.
- In stage IIIA,
- cancer has spread to the muscle layer and to 7 to 15 nearby lymph nodes; or
- cancer has spread to the subserosa and to 3 to 6 nearby lymph nodes; or
- cancer has spread to the serosa and to 1 to 6 nearby lymph nodes; or
- cancer has spread to nearby organs, such as the spleen, colon, liver, diaphragm, pancreas, abdomen wall, adrenal gland, kidney, or small intestine, or to the back of the abdomen.
- In stage IIIB,
- cancer may have spread to the submucosa or to the muscle layer and has spread to 16 or more nearby lymph nodes; or
- cancer has spread to the subserosa or to the serosa and has spread to 7 to 15 nearby lymph nodes; or
- cancer has spread to nearby organs, such as the spleen, colon, liver, diaphragm, pancreas, abdomen wall, adrenal gland, kidney, or small intestine, or to the back of the abdomen. Cancer has also spread to 1 to 6 nearby lymph nodes.
- In stage IIIC,
- cancer has spread to the subserosa or to the serosa, and to 16 or more nearby lymph nodes; or
- cancer has spread to nearby organs, such as the spleen, colon, liver, diaphragm, pancreas, abdomen wall, adrenal gland, kidney, or small intestine, or to the back of the abdomen. Cancer also has spread to 7 or more nearby lymph nodes.
Learn about treatment of stage III stomach cancer.
Stage IV (also called stage 4) stomach cancer
In stage IV, cancer has spread to other parts of the body, such as the lungs, liver, distant lymph nodes, and the tissue that lines the abdomen wall.
Stage IV stomach cancer is also called metastatic stomach cancer. Metastatic cancer happens when cancer cells travel through the lymphatic system or blood and form tumors in other parts of the body. The metastatic tumor is the same type of cancer as the primary tumor. For example, if stomach cancer spreads to the lung, the cancer cells in the lung are actually stomach cancer cells. The disease is called metastatic stomach cancer, not lung cancer. Learn more in Metastatic Cancer: When Cancer Spreads.
Learn about treatment of stage IV stomach cancer.
Recurrent stomach cancer
Recurrent stomach cancer is cancer that has recurred (come back) after it has been treated. Stomach cancer may come back in the stomach, lymph nodes, or other parts of the body, such as the liver, lung, or bone. Tests will be done to help determine where the cancer has returned in your body. The type of treatment that you have for recurrent stomach cancer will depend on where it has come back.
Learn more in Recurrent Cancer: When Cancer Comes Back. Information to help you cope and talk with your health care team can be found in Coping with Stomach Cancer and the booklet When Cancer Returns.


This information does not replace the advice of a doctor. Ignite Healthwise, LLC disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the Terms of Use and Privacy Policy. Learn how we develop our content.
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.